A 42 year female with multiple health issues.
G sai tejaswini
I have been given this case to solve in attempt and to understand the topic of patient clinical data analysis to develop my competency in reading and comprehending clinical data including history, clinical findings, investigations and come up with treatment plan.
Entire real patient clinical problems in this link herehttps://classworkdecjan.blogspot.com/2019/05/42-f-with-severe-regular-edema-with_17.html?m=1
Following is my analysis of the patient problem.
Problems are
INVESTIGATIONS: EEG
TREATMENT :Lserine induces sleep, cimetidine
OLIGURIA: due to G6PD deficiency there is oxidative stress causing kidney damage (reduced production of NADPH&ATP may lead to loss of ions and decreased urine production). It may be due to WNK1 gene mutation , kidney infections.
INVESTIGATIONS:CUE ,USG
Rashes:she was diagnosed as behcets syndrome which is an auto immune disorder which causes vasculitis, rashes, burred vision(improperblood supply to optic nerve).
INVESTIGATIONS:parthergy test , OCT, skin prick test.
HEAD ACHES:migraine with aura is associated with left sided numbness, left sided spinning movement, memory loss , vision loss.
Differential diagnosis :
Meningitis , encephalitis(no fever)
Brain tumors
Vestibular disorders
Cerebellar disorders
Stroke .
INVESTIGATIONS:EEG,MRI,CTscan,CSF analysis.
TREATMENT:guven-triptamines
Recomended-stay in dark room ,avoid stress
Drugs which triggers the condition and triptans acetaminophen, ergots.
Fatigue: due to G6PD deficiency causes decreased production of ATP so there is fatigue.
Aggrevated on exertion and stress.
TREATMENT:ribose Which generates ATP
OTHER PROBLEMS :PCOD, fractures, loss of hair, excessive growth of hair on the body , osteoarthritis anihydrosis(due WNK1gene mutation).
REFERENCES:https://classworkdecjan.blogspot.com/2019/05/42-f-with-severe-regular-edema-with_17.html?m=1
Roll no 61
I have been given this case to solve in attempt and to understand the topic of patient clinical data analysis to develop my competency in reading and comprehending clinical data including history, clinical findings, investigations and come up with treatment plan.
Entire real patient clinical problems in this link herehttps://classworkdecjan.blogspot.com/2019/05/42-f-with-severe-regular-edema-with_17.html?m=1
Following is my analysis of the patient problem.
Problems are
- Swelling of face and abdomen
- Sleep disturbances
- Oliguria
- Rashes
- Headaches(migraine with aura)
- Fatigue
Swelling of face and abdomen: she was diagnosed as G6PD deficiency which cauese hemolytic anemia ie hemolysis of rbc may cause right heart failure which may be the cause of shortness of breath and swelling .
Swelling of face may be caused due renal failure (oxidative stress due G6PD deficiency). This deficiency causes decreased generation ofNADPH and ATP which causes oxidative stress. These patients may have neonatal jaundice. Hiatus hernia may cause shortness of breath.
Aggrevating factors: fava beans,antimalarial drugs
INVESTIGATIONS:done -
CBP- anemia
LFT-AST,ALT levels increased.
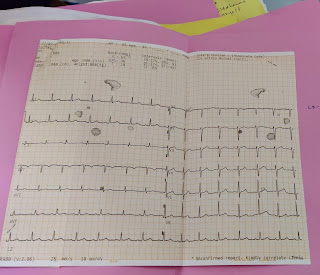
ECG- left atrial enlargement , right heart enlargement
Echocardiography.
Recomended:LDH LEVELS,serum haptaglobulin levels, peripheral blood smear.
TREATMENT:given -cimetidine , ribose(generation of ATP).
Recomended-blood transfusion ,o2 therapy.
SLEEP DISTURBANCES: G6PD deficiency cause impaired genaration of glycine which causes imapairment in seratonin level so thwre are sleep disturbances. This may be due to AMPD1 deficiency as adenosine inhibitory neurotransmitter is defective.
INVESTIGATIONS: EEG
TREATMENT :Lserine induces sleep, cimetidine
OLIGURIA: due to G6PD deficiency there is oxidative stress causing kidney damage (reduced production of NADPH&ATP may lead to loss of ions and decreased urine production). It may be due to WNK1 gene mutation , kidney infections.
INVESTIGATIONS:CUE ,USG
Rashes:she was diagnosed as behcets syndrome which is an auto immune disorder which causes vasculitis, rashes, burred vision(improperblood supply to optic nerve).
INVESTIGATIONS:parthergy test , OCT, skin prick test.
HEAD ACHES:migraine with aura is associated with left sided numbness, left sided spinning movement, memory loss , vision loss.
Differential diagnosis :
Meningitis , encephalitis(no fever)
Brain tumors
Vestibular disorders
Cerebellar disorders
Stroke .
INVESTIGATIONS:EEG,MRI,CTscan,CSF analysis.
TREATMENT:guven-triptamines
Recomended-stay in dark room ,avoid stress
Drugs which triggers the condition and triptans acetaminophen, ergots.
Fatigue: due to G6PD deficiency causes decreased production of ATP so there is fatigue.
Aggrevated on exertion and stress.
TREATMENT:ribose Which generates ATP
OTHER PROBLEMS :PCOD, fractures, loss of hair, excessive growth of hair on the body , osteoarthritis anihydrosis(due WNK1gene mutation).
REFERENCES:https://classworkdecjan.blogspot.com/2019/05/42-f-with-severe-regular-edema-with_17.html?m=1

Cite the references numbered in the text of your write up instead of mentioning Wikipedia at the bottom. Which statements made in your write up are from Wikipedia? 🤔
ReplyDeleteIs oliguria due to hemolysis her current problem?
ReplyDeleteAren't you supposed to solve her current problems currently? Why offer solutions now for a problem that was in the past? Do you think she still continues to have oliguria due to ongoing hemolysis? Would that be possible? When did she have oliguria?